Introduction
Methicillin-resistant Staphylococcus aureus is known to be a frequent source of recurrent infections and often a cause of ill infants at the neonatal intensive care units. The neonates have been shown to be vulnerable to these infections. Many studies have identified these risks associated and the exposure the infants have and the need for urgent attention to managing it (Friães et al., 2015 pp. 746). MRSA infection has been shown to be life-threatening in various cases. Staphylococcus bacteria affect children with weak immunity, and over the decades, studies have shown that MRSA has developed resistance from various anti bacteria management. This strain is often spread through spread and contact with surgical and invasive devices such as the implanted feeding tubes and surgical wounds (Tan et al., 2012). Neonates unit has become an avenue for colonization of the strain. It has often at times been spread horizontally through health care staff through healthcare-associated transmission through contact. Various have been implanted to control these outbreaks including hand hygiene main practices, active surveillance, implementation of isolation practices, contact isolation of subjects among other strategies (Rajam et al., 2011).
Aim
The study assesses genotype and culture approach investigating MRSA presents. The aim of this study protocol is to investigate Methicillin-resistant Staphylococcus aureus (MRSA) infection in Neonatal Intensive Care Unit.
Methods
The work was done according to the schedules provided.
Results
Graham Statin assessment
Table 1Experimental information
| Run Name | Two Step |
| Run Start | 07/03/2019 18:04:28 |
| Run Finish | 07/03/2019 19:02:53 |
| Operator | Dr Kimmitt |
| Notes | 6BIOM005W |
| Run On Software Version | Rotor-Gene 1.7.94 |
| Run Signature | The Run Signature is valid. |
| Gain Green | 5. |
Table 2 Graphical representation on Graham statin assessment
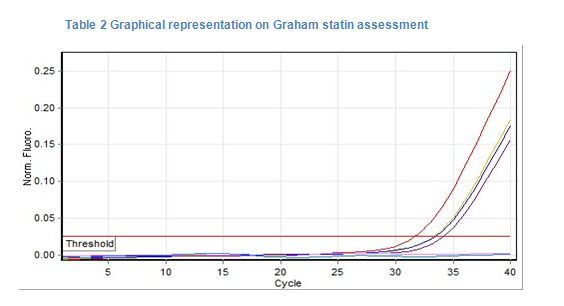
| No. | Colour | Name | Type | Ct | Given Conc (Copies) | Calc Conc (Copies) | % Var |
| 1 | PN | Unknown | 31.77 | ||||
| 2 | PS | Unknown | 33.34 | ||||
| 3 | + | Positive Control | 33.51 | ||||
| 4 | + | Positive Control | 34.21 | ||||
| 5 | Neg | Negative Control | |||||
| 6 | Neg | Negative Control |
Graham statin assessment revealed positive control culture with the blood swaps used in the task. The Chromogenic agar media is essential in isolating, identifying and differentiating various microorganisms. The medium has Chromogenic substrates which are utilized by the microorganism. Further, based on the color changes the colonies test positive for MRSA Colonization. The classical assessment of the media depends on the principle of ph color while the media is based on the utilization of the chromogenic substrates.
| TEST | RESULT |
| Gram stain | Gram positive coccus |
| Motility | Non-motile |
| Growth in air/anaerobically | Facultative anaerobe |
| Catalase | Positive |
| Glucose (acid) | Positive |
| Carbohydrates | Fermentative |
The results test positive control for graham positive on the blood swaps collected. This reflects the presence of colonies which need to be investigated throughout. The isolation of MRSA is often achieved through the use of culture specimens on general media purpose such as the blood agar with other subsequent identification can be done based on colonies and serological tests. This often involves tests of colonies based on the agglutination of Staphylococcus aureus.
More often Chromogenic media has been utilized on the isolation and detection of Staphylococcus aureus. CHROMagar is a selective media essential in a combination of chromogenic enzymes substrates which grow as mauve colonies. The detection of positive identification of MRSA is of great significance (Milstone et al., 2011). The use of selective media identifies a positive result for the graham positive bacteria signify further assessment on the blood swaps of the infant towards investigating the possible outbreak of MRSA in NICU (Campos et al., 2012 pp. 185). Thus the results showed the positive presence of graham positive cocci in the colonies present.
The PCR results obtained showed the presence of MRSA strain being identical from both culture sources signifying the presence of MRSA.
Bioinformatics analysis was undertaken on the culture
The blood samples collected from the infant were passed through genome tool to predict the protein analysis for possible identity. Assessment of single base changes on the genomes inferred transmission and presence of infections. The two runs indicated the presence of MRSA as the alignment scores were similar for the two runs conducted. The sequencing isolates obtained indicate that they share the same color, a small genetic difference could be noted form the sample tests suggesting a carrier. The results below indicate identical swab results having the characterization of the MRSA and the connection to its relatedness on the phylogenetic features signifying outbreak.
The results above indicate that there is an MRSA colonization taking place. The gene strap run on the samples signifies a positive presence. The genome analysis from the two blood sites isolate the blood and umbilical cord isolates display a similar genome pattern as indicated above.
Staphylogeny results of the swabs
Figure 2 Staphylogeny results of the swab
The results of the styphylogeny run above indicate that there is a presence of MRSA infection outbreak from the newborn unit. The figures above indicate the infant sepsis taking on different direction while the strains moving upwards indicating an outbreak elsewhere not in the NICU.
Whole sequence genome for MRSA is key in identifying transmission of the infection is key in establishing the source of the strain infection. The phylogenetic analysis shows strain outbreak infection transmitted through a carrier outbreak outside the hospital set up.
Drug anti microbial resistance assessment
Table 2: Results of disc susceptibility testing of the case study strain.
Blood culture
| Antibiotic (Disc content) | Clinical Breakpoint | Case study strain; Staphylococcus aureus | S or R |
| Inhibition zone diameter in mm | |||
| Cefoxitin FOX 30µg | 24 | No inhibition | R |
| Norfloxacin NOR 10µg | 20 | No inhibition | R |
| Tobramycin TOB 10µg | 32 | No inhibition | R |
| Erythromycin E 15µg | 21 | 11.21 | R |
| Clindamycin DA 2µg | 35 | 26.77 | R |
| Fusidic acid FD 10µg | 24 | 34.10 | S |
Umbilical cord
| Antibiotic (Disc content) | Clinical Breakpoint | Case study strain; Staphylococcus aureus | S or R |
| Inhibition zone diameter in mm | |||
| Cefoxitin FOX 30µg | 24 | 11 | R |
| rNrorfloxacin NOR 10µg | 20 | NO growth | R |
| Tobramycin TOB 10µg | 32 | 30 | R |
| Erythromycin E 15µg | 21 | No growth | R |
| Clindamycin DA 2µg | 35 | 34.8 | R |
| Fusidic acid FD 10µg | 24 | 42 | S |
The minimum inhibitory concentration (MIC) means the lowest concentration of an antibiotic that will inhibit the visible growth of a microorganism after overnight incubation
Table 4: Results of MIC of the case study strain.
Blood culture
| Antibiotic | MIC |
| Oxacillin | 256+ |
| Vancomycin | 4 mg/L |
Umbilical cord
| Antibiotic | MIC |
| Oxacillin | 256+ |
| Vancomycin | 5 |
Table 5; Results of disc susceptibility testing of the case study strain.
Blood culture
| Antibiotic (Disc content) | Clinical Breakpoint | Case study strain; Staphylococcus aureus | S or R |
| Inhibition zone diameter in mm | |||
| Cefoxitin FOX 30µg | 24 | No inhibition | R |
| Norfloxacin NOR 10µg | 20 | No inhibition | R |
| Tobramycin TOB 10µg | 32 | No inhibition | R |
| Erythromycin E 15µg | 21 | 11.21 | R |
| Clindamycin DA 2µg | 35 | 26.77 | R |
| Fusidic acid FD 10µg | 24 | 34.10 | S |
Umbilical cord
| Antibiotic (Disc content) | Clinical Breakpoint | Case study strain; Staphylococcus aureus | S or R |
| Inhibition zone diameter in mm | |||
| Cefoxitin FOX 30µg | 24 | 11 | R |
| norfloxacin NOR 10µg | 20 | NO growth | R |
| Tobramycin TOB 10µg | 32 | 30 | R |
| Erythromycin E 15µg | 21 | No growth | R |
| Clindamycin DA 2µg | 35 | 34.8 | R |
| Fusidic acid FD 10µg | 24 | 42 | S |
Discussion
Treatment management
Determining the susceptibility of the strains to antibiotics reveal some clinical perspectives which are essential for managing the MSRA. Zone point assessment was used to determine to resistance and susceptibility nature of the bacteria. The two blood samples culture was used to test the resistance and susceptibility of the drugs to the MRSA. Inhibition zone was effective in determining the nature of treatment. Smaller inhibition size identified resistance while bigger inhibition size reflected susceptibility (Dezfulian et al., 2012).
Management of MRSA has shown resistance to various antibiotics. The study showed the resistance of MRSA to various anti microbe’s drugs.
The results above indicate that management using Fusidic acid is able to counter the infectious strain of MRSA currently being witnessed in the NICU. As indicated the results showed no effect with high resistance to the MRSA.
The two sets of the results used; the blood culture and the umbilical assessment showed similar trends on drug response. The resistance developed from the two swabs above shows similar trends thus signifying the effectiveness of Fusidic acid 10 µg as an effective source of treatment.
Further, assessment of MIC indicates that Oxacillin has an effective MIC assessment on the patient. Thus usage of Oxicillin will be effective in managing multi-drug resistant Staphylococcus Aureus.
Outbreak analysis
The assessment of an outbreak from the NICU shows that there is an occurrence of an outbreak however not originating from the NICU. The phylogeny tree diagram shows that the outbreak source is outside NICU and has long traces. The neonate is part of any identifiable cluster which has traces of MRSA. This indicates significant steps to be taken b the NICU infection control team. There is a need to raise awareness and enhance surveillance and prevention protocol practices. Screening of staff needs to be initiated so that the carriers can be tested and managed for prevention (Pacheco et al., 2011).
Research studies have indicated that the use of gloves and masks for contact among hospitalized patients have been sued (Milestone et al., 2011). Further use of anti germs agents such as mupirocin ointment has been used tremendously to reduce infection control among nasal carriers. Further adoption and maintenance on the sue gloves, hand hygiene and use of cleaning disinfectant have been recommended as proven strategies to improve on the disease control (Calfee et al., 2014).
Chromogenic Media vs Real-Time PCR for Nasal Surveillance of Methicillin-Resistant Staphylococcus aureus
Surveillance and control of MRSA are vital in infection control management. The sensitivity employed during assessments affects the isolation captures thus determining the failures of MRSA control management. between the use of Chromogenic culture and real-time PCR, real-time PCR provided faster results due to high sensitivity associated with it compared to chromogenic culture, (78.5%–98.2%), specificities (91.6%–100.0% (Paule et al., 2009). Based on the preference of PCR, the NICU is able to conduct rapid assessment son its NICU staff to establish the carriers for effective isolation process.
PCR has an advantages effect in that it allows for a faster way of identifying the strain much faster compared to the chromogenic culture. Further, the latter is prone to infection and hence its reliability can be at times not correct leading to wrong identification of true positives in a sample.
Conclusion
MRSA infection is a public health hazard and has significant effects especially at NICU due to weak immune systems associated with children. the resistance developed has made it impossible for effective eradication of the strain. The assessment at the NICU investigated has shown that the strain of MRSA is present at NICU. Staphylogenic assessment reveals mutation however not sourced from the NICU. There is a possibility of carrier among the staff at the NICU. The most effective drug to be offered is Fusidic acid FD 10µg. There is a need to conduct an analysis of the NICU using PCR analysis tool as it offered reliable results for the identification of the strain. In view of this, the infection control team need to roll out a control program of hand hygiene and use of disinfectants to improve hygiene and carry out surveillance in the NICU to prevent further spread.
This study examined infection associated with the umbilical cord in neonatal ward. The inflammation and consequential sepsis of the umbilical cord leads to health complicated challenges on the infant. This practical assessed neonate infection with sepsis having secondary infection. Occurrence of sepsis can lead to complication and embolization leading to metastatic foci of the organs. In normal cases the standards treatment procedures entail administration of anti biotic drugs. Current treatment options entail medication options such as tetracycline, rifampicin, linezolid, clindamycin, trimethropin and sulfamethoxazole. Treatments are often based on the type of infection, location and severity of symptoms.
Effective management of the infection entail combination management of parental administration of antiphylococcal penicillin and aminoglycoside anti biotic for non complicated cases while complicated cases involve requires more aggressive process with application of antimicrobial therapy of Metronidazole combined with ant staphylococcal penicillin and aminoglycosid.
Application of anti microbial agents can be initiated to recued bacterial colonization and prevent further sepsis states. Vancomyicicn is recommended while intervention dosage of 15mg/kg /dose every 6 hours is recommended for maintenance of the drug at a dosage of 15-20 ug/mL level.
There exist two types of MRSA infections in the ward. Health care associated and community based associated MRSA. This assessments shows community based infection of MRSA leading to the NICU. Community based MRSA are contracted outside health care setting. Its prevention in both is maintenance of hygiene practices and individual living environments. In the ward there are various MRSA infections. Environmental and physical contact infections of MRSA do exist. Prevention is to ensure hand hygiene practices are implemented and contamination minimised in the ward.
The case study incidence reflects community based infection of MRSA.. Genotype MRDA investigation is key due to its sensitivity, speed and low cost method for typing MRSA. In culture method, key nutrients are applied to the bacteria to allow the bacteria to grow thus taking significant loner duration of time. Then the bacterium is culture and observed thereafter. This method is often long and expensive thus it prolongs diagnosis periods.
In the practical al the protocol procedures were undertaken with regard to culture method application. From this assessment genotype investigation is the best method of investigating MRSA outbreak. The most referred method of treatment for infants is the application of anti microbial ointments on the umbilical site. This is essential to ensure that anti bacteria toxicity is not build on the neonate’s body.
References
Calfee, D.P., Salgado, C.D., Milstone, A.M., Harris, A.D., Kuhar, D.T., Moody, J., Aureden, K., Huang, S.S., Maragakis, L.L. and Yokoe, D.S., 2014. Strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in acute care hospitals: 2014 update. Infection Control & Hospital Epidemiology, 35(7), pp.772-796.
Campos, G.B., Souza, S.G., Lobão, T.N., Da Silva, D.C., Sousa, D.S., Oliveira, P.S., Santos, V.M., Amorim, A.T., Farias, S.T., Cruz, M.P. and Yatsuda, R., 2012. Isolation, molecular characteristics and disinfection of methicillin-resistant Staphylococcus aureus from ICU units in Brazil. New Microbiologica, 35(2), pp.183-190.
Dezfulian, A., Aslani, M.M., Oskoui, M., Farrokh, P., Azimirad, M., Dabiri, H., Salehian, M.T. and Zali, M.R., 2012. Identification and characterization of a high vancomycin-resistant Staphylococcus aureus harboring VanA gene cluster isolated from diabetic foot ulcer. Iranian journal of basic medical sciences, 15(2), p.803.
Friães, A., Resina, C., Manuel, V., Lito, L., Ramirez, M. and Melo-Cristino, J., 2015. Epidemiological survey of the first case of vancomycin-resistant Staphylococcus aureus infection in Europe. Epidemiology & Infection, 143(4), pp.745-748.
Milstone, A.M., Goldner, B.W., Ross, T., Shepard, J.W., Carroll, K.C. and Perl, T.M., 2011. Methicillin-resistant Staphylococcus aureus colonization and risk of subsequent infection in critically ill children: importance of preventing nosocomial methicillin-resistant Staphylococcus aureus transmission. Clinical infectious diseases, 53(9), pp.853-859.
Pacheco, R.L., Lobo, R.D., Oliveira, M.S., Farina, E.F., Santos, C.R., Costa, S.F., Padoveze, M.C., Garcia, C.P., Trindade, P.A., Quiterio, L.M. and Rivitti, E.A., 2011. Methicillin-resistant Staphylococcus aureus (MRSA) carriage in a dermatology unit. Clinics, 66(12), pp.2071-2077.
Paule, S.M., Mehta, M., Hacek, D.M., Gonzalzles, T.M., Robicsek, A. and Peterson, L.R., 2009. Chromogenic media vs real-time PCR for nasal surveillance of methicillin-resistant Staphylococcus aureus: impact on detection of MRSA-positive persons. American journal of clinical pathology, 131(4), pp.532-539.
Rajam, G., Hammons, G.M., Carlone, G.M., Sampson, J.S. and Ades, E.W., 2011. A novel innate immune-enhancement strategy combined with IVIG rescues mice from fatal Staphylococcus aureus septicemia. Clin. Vaccine Immunol., 17(11), pp.1823-1824.
Tan, C.M., Therien, A.G., Lu, J., Lee, S.H., Caron, A., Gill, C.J., Lebeau-Jacob, C., Benton-Perdomo, L., Monteiro, J.M., Pereira, P.M. and Elsen, N.L., 2012. Restoring methicillin-resistant Staphylococcus aureus susceptibility to β-lactam antibiotics. Science Translational Medicine, 4(126), pp.126ra35-126ra35.